
What is an anal abscess?
An anal abscess is an infected cavity filled with pus found near the anus or rectum.
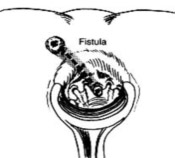 What is an anal fistula?
What is an anal fistula?
An anal fistula (also called fistula-in-ano) is frequently the result of a previous or current anal abscess, occurring in up to 50% of patients with abscesses. Normal anatomy includes small glands just inside the anus. Occasionally, these glands get clogged and potentially can become infected, leading to an abscess. The fistula is a tunnel that forms under the skin and connects the infected glands to the abscess. A fistula can be present with or without an abscess and may connect just to the skin of the buttocks near the anal opening. Other situations that can result in a fistula include Crohn’s disease, radiation, trauma and malignancy.
How does someone get an anal abscess or a fistula?
The abscess is most often a result of an acute infection in the internal glands of the anus. Occasionally, bacteria, fecal material or foreign matter can clog the anal gland and create a condition for an abscess cavity to form. Other medical conditions can make these types of infections more likely.
After an abscess drains on its own or has been drained (opened), a tunnel (fistula) may persist, connecting the infected anal gland to the external skin. This typically will involve some type of drainage from the external opening and occurs in up to 50% of abscesses. If the opening on the skin heals when a fistula is present, a recurrent abscess may develop.
What are the specific signs or symptoms of an abscess or fistula?
A patient with an abscess may have pain, redness or swelling in the area around the anal area. Fatigue, general malaise, as well as accompanying fever or chills are also common. Similar signs and symptoms may be present when patients have a fistula, with the addition of possible irritation of the perianal skin or drainage from an external opening.
Is any specific testing necessary to diagnose an abscess or fistula?
No. Most anal abscesses or fistula-in-ano are diagnosed and managed on the basis of clinical findings. Occasionally, additional studies such as ultrasound, CT scan, or MRI can assist with the diagnosis of deeper abscesses or the delineation of the fistula tunnel to help guide treatment.
What is the treatment of an anal abscess?
The treatment of an abscess is surgical drainage under most circumstances. An incision is made in the skin near the anus to drain the infection. This can be done in a doctor’s office with local anesthetic or in an operating room under deeper anesthesia. Hospitalization may be required for patients prone to more significant infections such as diabetics or patients with decreased immunity.
Are antibiotics required to treat this type of infection?
Antibiotics alone are a poor alternative to drainage of the infection. For uncomplicated abscesses, the addition of antibiotics to surgical drainage does not improve healing time or reduce the potential for recurrences. There are some conditions in which antibiotics are indicated, such as for patients with compromised or altered immunity, some cardiac valvular conditions or extensive cellulitis. A comprehensive discussion of your past medical history and a physical exam are important to determine if antibiotics are indicated.
What is the treatment of an anal fistula?
Surgery is almost always necessary to cure an anal fistula. Although surgery can be fairly straightforward, it may also be complicated, occasionally requiring staged or multiple operations. Consider identifying a specialist in colon and rectal surgery who would be familiar with a number of potential operations to treat the fistula.
The surgery may be performed at the same time as drainage of an abscess, although sometimes the fistula doesn’t appear until weeks to years after the initial drainage. If the fistula is straightforward, a fistulotomy may be performed. This procedure involves connecting the internal opening within the anal canal to the external opening, creating a groove that will heal from the inside out. This surgery often will require dividing a small portion of the sphincter muscle, which has the unlikely potential for affecting the control of bowel movements in a limited number of cases.
Other procedures include placing material within the fistula tract to occlude it or surgically altering the surrounding tissue to accomplish closure of the fistula, with the choice of procedure depending upon the type, length, and location of the fistula. Most of the operations can be performed on an outpatient basis, but may occasionally require hospitalization.
What is the recovery like from surgery?
Pain after surgery is controlled with pain pills, fiber and bulk laxatives. Patients should plan for time at home using sitz baths and attempt to avoid the constipation that can be associated with prescription pain medication. Discuss with your surgeon the specific care and time away from work prior to surgery to prepare yourself for post-operative care.
Can the abscess or fistula recur?
If adequately treated and properly healed, both are unlikely to return. However, despite proper and indicated open or minimally invasive treatment, both abscesses and fistulas can potentially recur. Should similar symptoms arise, suggesting recurrence, it is recommended that you find a colon and rectal surgeon to manage your condition.
What is a colon and rectal surgeon?
Colon and rectal surgeons are experts in the surgical and non-surgical treatment of diseases of the colon, rectum and anus. They have completed advanced surgical training in the treatment of these diseases as well as full general surgical training. Board-certified colon and rectal surgeons complete residencies in general surgery and colon and rectal surgery, and pass intensive examinations conducted by the American Board of Surgery and the American Board of Colon and Rectal Surgery. They are well versed in the treatment of both benign and malignant diseases of the colon, rectum and anus and are able to perform routine screening examinations and surgically treat conditions if indicated to do so.
author: Michael Buckmire, MD, FACS, FASCRS, on behalf of the ASCRS Public Relations Committee – © 2012 American Society of Colon & Rectal Surgeons